Cerebral palsy is an umbrella term for a group of permanent disorders that affect movement and/or posture and motor function. It is one of the most common and severe disabilities in childhood.
What is Cerebral Palsy?
Cerebral Palsy affects the brain’s ability to control muscles. It is caused by injury to a developing brain that control movement, balance, and posture. This injury can occur during pregnancy, childbirth, or early childhood. CP varies in severity and can affect muscle tone, coordination, and motor skills. It does not worsen over time, but the symptoms may change as a child grows. CP may coexist with other conditions, such as epilepsy or learning disabilities. Treatment aims to improve mobility, manage symptoms, and support the child’s development.
What Are the Types of Cerebral Palsy?
Cerebral Palsy (CP) encompasses several different types, each characterised by specific movement and coordination challenges. Here are the primary types:
Spastic Cerebral Palsy
This is the most common type, affecting approximately 70% of individuals with CP.
It causes stiffness and tightness in muscles, leading to difficulty in movement and range of motion.
Subtypes include:
- Spastic hemiplegia – One side of the body is affected, usually arm is more affected than the leg.
- Spastic diplegia – Both legs are more affected than the arms.
- Spastic quadriplegia – All four limbs are affected, often with severe involvement of the arms and legs.
Dyskinetic Cerebral Palsy
- It includes dystonic, athetoid or choreoathetoid CP.
- It involves involuntary movements, such as twisting, writhing, or jerking motions.
- Individuals may have difficulty controlling their posture and may experience fluctuations in muscle tone, alternating between stiffness and floppiness.
Mixed Cerebral Palsy
- Some individuals with CP may have symptoms that do not fit neatly into one type but exhibit characteristics of multiple types.
- For example, a person may have both spasticity and dyskinesia.
Ataxic Cerebral Palsy
- Ataxia means poor balance, or without coordination
- Definition and description of ataxic CP is generally lacking
- High proportion of people with ataxic CP has an incorrect initial diagnosis
- All children presented with early onset ataxia or ataxic CP should be assessed by Paediatric Neurologist.
Hypotonic Cerebral Palsy
- Hypotonic means low tone
- High proportion of people with hypotonic CP has an incorrect initial diagnosis
- All children presented with axial or peripheral hypotonia or hypotonic CP should be assessed by Paediatric Neurologist.
What Causes Cerebral Palsy?
Cerebral Palsy (CP) is caused by abnormal development or injury to a developing brain, particularly in areas that control movement, balance, and posture. The exact cause of CP can vary and may not always be known. However, several factors can contribute to the development of CP:
Before Birth
- Abnormal brain development during pregnancy can occur due to genetic disorders, infections, maternal health conditions, or exposure to toxins or radiation.
- Infections during pregnancy, such as rubella (German measles), cytomegalovirus (CMV), or toxoplasmosis, can increase the risk of CP.
- Certain maternal health conditions, such as thyroid disorders or diabetes, can affect fetal brain development and increase the risk of CP.
During Birth
- Oxygen deprivation or trauma during labour and delivery, such as umbilical cord complications, placental abruption, or prolonged labour, can lead to brain damage and CP.
- Premature infants are at higher risk of CP due to their immature and vulnerable brain development.
After Birth
- Traumatic brain injuries, infections (such as meningitis or encephalitis), or other acute neurological conditions occurring after birth can result in CP.
- Stroke in infants or young children can cause brain damage, leading to CP.
- Untreated severe jaundice (hyperbilirubinemia) in newborns can lead to a type of brain damage called kernicterus, resulting in dyskinestic CP.
What Are the Signs and Symptoms of Cerebral Palsy?
Cerebral Palsy (CP) can present with a variety of signs and symptoms, which may vary in severity and combination from one individual to another. Some common signs and symptoms of CP include:
Delayed Milestones
- Traumatic brain injuries, infections (such as meningitis or encephalitis), or other acute neurological conditions occurring after birth can result in CP.
- Stroke in infants or young children can cause brain damage, leading to CP.
- Untreated severe jaundice (hyperbilirubinemia) in newborns can lead to a type of brain damage called kernicterus, resulting in dyskinestic CP.
Abnormal Muscle Tone
- Spasticity – Muscle stiffness or tightness
- Dystonia – Involuntary muscle spasms, repetitive awkward and twisting posture
- Athetosis – Involuntary slow, flowing, writhing, worm-like movement
- Chorea – Involuntary rapid, irregular, excessive, dance-like movement
- Ballimus – involuntary rapid, violent flinging movement
Abnormal Reflexes
- Persistent primitive reflexes beyond infancy, such as the Moro reflex (startle reflex) or Asymmetric Tonic Neck Reflex (ATNR).
- Exaggerated deep tendon reflexes in response to stimuli or tendon hammer.
Coordination and Balance Difficulties
- Weak arms or legs
- Fidgety, jerky or clumsy movement
- Random, uncontrolled movement
Gait Abnormalities
- Scissoring – Legs cross or “scissor” when walking due to tight muscles (dystonia)
- Toe walking – Walking on tiptoes instead of using a typical heel-to-toe pattern.
Speech and Swallowing Difficulties
- Dysarthria – Difficulty with articulation and control of speech muscles, leading to slurred or unclear speech.
- Dysphagia – Difficulty with swallowing, which may result in choking or aspiration.
Other Symptoms
- Seizures & Epilepsy – 25% of children with CP may experience epileptic seizures, which can vary in type and severity.
- Learning Disabilities – While CP primarily affects movement and posture, some individuals may also have cognitive impairments or learning disabilities.
What Are The Common Co-Occurring Conditions?
Individuals with Cerebral Palsy (CP) may experience a variety of co-occurring conditions that can impact their overall health and well-being. Some common co-occurring conditions include:
Cognitive impairment
While CP primarily affects movement and posture, 25% of children with CP may also have learning disabilities or cognitive impairments that affect learning, problem-solving, and adaptive functioning.
Epilepsy and Epileptic Seizures
25% of children with CP may experience seizures. These seizures can vary in type and severity and may require treatment with anti-seizure medications.
Speech and Communication difficulties
CP can affect the muscles involved in speech and communication, leading to difficulties with articulation, clarity, and fluency in up to 40% of children with CP. Speech and language therapy may be beneficial in improving communication skills.
Vision Impairment
40% of children with CP have visual impairments, which may include strabismus (crossed eyes), nystagmus (involuntary eye movements), or cortical visual impairment. Regular ophthalmological assessment and interventions may be necessary.
Hearing Impairment
9% of children with CP may also experience hearing impairments, either due to congenital factors, complications of prematurity, or repeated ear infections. Hearing assessment and appropriate interventions are essential for optimal communication and development.
Gastrointestinal Issues
Digestive problems such as gastroesophageal reflux disease (GERD), constipation, or difficulty swallowing (dysphagia) are common in individuals with CP. Proper management and dietary modifications may be necessary to address these issues.
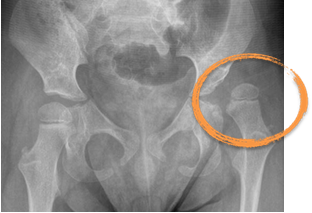
Orthopaedic Complications
Up to 20% of children with CP can lead to musculoskeletal issues such as hip subluxation/ dislocation, scoliosis,and joint deformities due to muscle stiffness or muscle weakness. Physical therapy, pharmacological treatments, orthotic devices or surgical interventions may be required to manage these complications.
Behavioural and Emotional Challenges
Living with a long term neurological condition like CP can impact emotional well-being and may contribute to behavioural and psycho-emotional challenges such as anxiety, depression, or social interaction difficulties. Counselling and psychosocial support can help address these issues.
Dental and Oral Health Problems
Individuals with CP may be at increased risk of dental caries, gum disease, or malocclusion (misalignment of teeth) due to factors such as poor oral hygiene, difficulty with oral care, or dental anomalies.
Sleep Disorders
Sleep disturbances such as sleep apnea, insomnia, or disrupted sleep patterns are more prevalent in children with CP (up to 15-20%) and may affect overall health and quality of life.
How to diagnose Cerebral Palsy?
Diagnosing Cerebral Palsy (CP) in children involves a thorough evaluation by paediatric neurologist, including medical history, physical examination, developmental assessment, and neurological evaluation. Diagnostic criteria based on clinical signs of motor impairments, abnormal muscle tone, and non-progressive motor dysfunction confirm the diagnosis.
Collaboration with multidisciplinary teams, including therapists and specialists, helps assess functional abilities and rule out other conditions. Family history and genetic testing may be considered to identify underlying genetic factors. Early detection and intervention are crucial for optimising outcomes and providing appropriate support for children with CP and their families.
What Are The Treatment Options For Cerebral Palsy?
Treatment options for Cerebral Palsy (CP) aim to manage symptoms, improve mobility and function, and enhance overall quality of life for individuals affected by the condition. Here are common treatment approaches:
Physical Therapy
Physical therapy focuses on improving muscle strength, flexibility, balance, and mobility through exercises and therapeutic techniques. It may also include training in activities of daily living and the use of assistive devices such as braces or walkers.
Occupational Therapy
Occupational therapy helps individuals develop skills for daily tasks, such as dressing, feeding, and writing, to promote independence and improve quality of life. It may involve adaptive equipment and techniques tailored to the individual’s needs.
Speech Therapy
Speech therapy addresses communication difficulties, swallowing problems (dysphagia), and oral motor issues commonly associated with CP. Therapists work to improve speech clarity, language skills, and swallowing function.
Medications
Medications may be prescribed to manage symptoms associated with CP, such as spasticity/ dystonia, seizures, pain, or gastrointestinal issues. Common medications include muscle relaxants, brain cell modulators, anti-seizure medications, pain relievers, and medications for reflux or constipation.
Botulinum Toxin Therapy (Botox)
Botulinum toxin therapy temporarily reduces muscle spasticity or dystonia, and it aims to improve the range of motion, preserve joint alignment, and to improve ease of comfort and care. They are commonly used in conjunction with physical and/or occupational therapy, serial casting and orthotic devices to facilitate stretching exercises, standing and functional activities.
Orthopaedic Interventions
Orthopaedic treatments may be necessary to address functional musculoskeletal deformities such as hip subluxation/ dislocation, contractures, scoliosis, or joint deformities.
Selective Dorsal Rhizotomy (SDR)
SDR is a neurosurgical procedure that involves cutting specific nerves in the spinal cord to reduce spasticity and improve mobility in selected children with CP.
Intrathecal Baclofen Therapy (ITB)
Spasticity can be treated with physiotherapy and oral medications such as Baclofen, but these are sometimes ineffective or have unacceptable side effects. Intrathecal baclofen treatment involves injecting medication into the cerebrospinal fluid which surrounds the spinal cord. A pump implanted in the abdomen injects baclofen into the cerebrospinal fluid, increasing the drug’s effectiveness and reducing adverse events.
Intrathecal baclofen (ITB) therapy has demonstrated a dramatic improvement in severe spasticity together with long-term safety.
Functional Electrical Stimulation (FES)
FES involves applying electrical stimulation to muscles to improve muscle strength, reduce spasticity, and promote functional movement, particularly in individuals with weak or paralysed muscles.
Alternative and Complementary Therapies
Alternative therapies, such as hippotherapy (horseback riding), aquatic therapy, acupuncture, or massage, may complement conventional treatments and promote relaxation, pain relief, and improved mobility.
References
Dr Yeo’s recent peer-group review journal publications and relevant articles regarding Cerebral Palsy (CP) and Long Term Neurological Conditions (LTNC):
Chia, Aletheia & Tan, Yi & Yeo, Tong & Teoh, Oon & Ng, Zhi Min. (2022). Epidemiology and risk factors for sleep disturbances in children and youth with cerebral palsy: An ICF-based approach. Sleep Medicine. 96. 10.1016/j.sleep.2022.04.021.
Leow, XYJ & Tan, JTC & Yeo, Tong & Wong, Kenneth & Mahadev, Arjandas & Ang, Bixia & Vasanwala, Rashida & Ng, Zhi Min. (2021). Evaluation of risk factors associated with fragility fractures and recommendations to optimise bone health in children with long-term neurological condition. Singapore Medical Journal. 64. 10.11622/smedj.2021124.
Ng, Zhi Min & Lin, Jeremy & Khoo, Poh & Rajadurai, Victor & Chan, Derrick & Ong, Hian & Wong, Janice & Choong, Chew & Lim, Kim & Lim, Kevin & Yeo, Tong. (2021). Causes, functional outcomes and healthcare utilisation of people with cerebral palsy in Singapore. Annals of the Academy of Medicine, Singapore. 50. 111-118. 10.47102/annals-acadmedsg.2020489.
KKH Hip Surveillance Programme for Children with Long term Neurological Conditions
Special Delivery, Issue 3, March 2018
(By Dr Ng Zhi MIn, Dr Yeo Tong Hong, A/Prof Arjandas Mahadev)
Special Delivery, Issue 3, March 2018
(By Dr Ng Zhi MIn, Dr Yeo Tong Hong, A/Prof Arjandas Mahadev)
Yeo TH, Brooks L, Differences in perceptions of palliative care needs for children with neurological conditions. Support Palliat Care 2012;2:A18.
Research Trials
– Co-investigator, Singapore Cerebral Palsy Registry, 2017 – ongoing research project
– Local principal investigator, Royal Hospital for Children, Glasgow, UKMCRN trial – ‘The efficacy, safety and tolerability of nabiximols (Sativex) as an adjunctive treatment to existing anti-spasticity medications in children aged 8 to 18 years with spasticity due to cerebral palsy who have not responded adequately to their existing anti-spasticity medications: a parallel group randomised, double-blind, placebo-controlled study’, 2014 – 2016.